
 Submit Manuscript
Submit Manuscript
Research Article | Open Access
Cervicovaginal foetal fibronectin in predicting success of induced labour among nulliparous women: a systematic review
Fawad Inayat1, Imad Tariq2, Nabiha Bashir3, Fawad Ullah4, Hadiqa Aimen5
1Department of Biochemistry, Institute of Chemical and Life Sciences, Abdul Wali Khan University, Mardan, 23200, Khyber Pakhtunkhwa, Pakistan.
2Department of Health and Biological Sciences, Abasyn University, Peshawar 25000, Khyber Pakhtunkhwa, Pakistan.
3Khwaja Fareed University of Engineering & Information Technology (KFUEIT), Rahim Yar Khan, 64200, Punjab, Pakistan.
4Michigan Technological University, 1400 Townsend Dr, Houghton, MI 49931, United States.
5COMSATS University Islamabad, Islamabad 44100, Islamabad, Pakistan.
Correspondence: Fawad Inayat (Department of Biochemistry, Institute of Chemical and Life Sciences, Abdul Wali Khan University, Turu Road, Near Sheikh Maltoon Town, Mardan, 23200, Khyber Pakhtunkhwa, Pakistan; E-mail: fawad.313b@gmail.com).
Asia-Pacific Journal of Surgical & Experimental Pathology 2024, 1: 28-35. https://doi.org/10.32948/ajsep.2024.08.01
Received: 02 May 2024 | Accepted: 19 Jul 2024 | Published online: 02 Aug 2024
Method A complete review of the literature was undertaken, including PubMed, EMBASE, Cochrane Library, and Google Scholar databases, with the search period extending until April 2023. The studies included in this analysis focused on investigating the predictive value of fetal fibronectin (fFN) concerning induced labor outcomes in nulliparous women. The process of data extraction primarily concentrated on the features of the study, interventions, controls, criteria for inclusion and exclusion, and the outcomes that were evaluated. The quality of the included studies was assessed using the Newcastle-Ottawa Scale.
Results The review synthesized findings from five studies, revealing varied predictive values of fFN. Sciscione et al. (2005) reported no significant difference in vaginal delivery rates between positive and negative fFN groups (Positive fFN: 55.8% vs. Negative fFN: 53.3%; P > .70). Uygur et al. (2016) found a higher cesarean section rate in patients with negative fFN results (P = 0.002). Reis et al. (2003) highlighted that higher parity and Bishop scores were more predictive than fFN alone (P = .021 for funneling; P = .157 for fFN presence). Grab et al. (2022) and Khalaf et al. (2023) further corroborated fFN's role in predicting labor outcomes, with the latter study demonstrating high sensitivity (85%), specificity (80%), and accuracy (82.6%) in predicting successful labor induction (P < .05 for Bishop score relation with fFN; P = 0.029 for positive vs. negative fFN).
Conclusion This systematic review validated that fFN is a significant biomarker for predicting labor induction outcomes, especially in nulliparous women. The combination of additional clinical factors with fFN has been shown to boost its prediction accuracy, indicating the need for a personalized strategy to labor induction.
Key words foetal fibronectin, nulliparous women, cervical length, ultrasonography
The determined function of fetal fibronectin (fFN) as a prognostic marker for preterm labor has been well-documented. The occurrence of this substance in cervicovaginal secretions after the mid-trimester stage is linked to a heightened likelihood of premature birth, indicating its potential usefulness in forecasting outcomes related to labor induction [3]. Numerous studies have investigated the association between heightened levels of fFN and diverse labor outcomes, including the efficacy of labor induction, length of labor, and the probability of vaginal birth as opposed to cesarean section [4, 5].
Furthermore, the use of quantitative evaluation of fFN, in conjunction with cervical length measurement by transvaginal ultrasonography, has emerged as an innovative method to enhance the accuracy of labor induction result prediction [6]. The combination has shown the potential to improve the precision of predictions, providing a more thorough evaluation of the cervix's preparedness for labor [7]. This method has significance not only because it has the potential to decrease needless medical interventions, but also because it can optimize the time for labor induction, leading to improved outcomes for both mothers and newborns [8].
Recent research has provided clinical professionals with useful insights into the chances of attaining vaginal birth by further defining the thresholds of fFN levels that are associated with effective labor induction [9]. These observations are vital for guiding clinical judgments, providing guidance to patients, and customizing induction techniques to suit individual requirements [10, 11]. Furthermore, studies have initiated investigations into the consequences of fFN levels concerning certain induction techniques, such as the administration of prostaglandins or mechanical methods like the Foley catheter, therefore enhancing a more individualized approach to labor induction [12, 13].
Labor induction is an essential procedure performed when the advantages of giving birth to the woman or fetus are greater than the dangers of extending the pregnancy [14]. Although this medical procedure is often performed, precisely predicting its results, especially in women who have not given birth and have an unfavorable cervix, continues to be a major obstacle [15]. Current developments in the field of obstetrics have been mostly focused on the identification of dependable prognostic indicators for the efficacy of labor induction. One of the glycoproteins that has received significant attention is fFN, which is in the extracellular matrix of the amniotic membrane [16, 17].
Nevertheless, despite the increasing amount of data that supports the usefulness of fFN in forecasting labor induction results, there are still obstacles that need to be addressed. Heterogeneity in results has been seen due to the variability in study designs, demographic characteristics, and methodology, highlighting the need for more research. The objective of this systematic review is to consolidate existing data on the predictive influence of fetal fibronectin on the outcome of labor induction in nulliparous women.
A thorough literature search was performed on several electronic databases, such as PubMed, EMBASE, Cochrane Library, and Google Scholar, covering the period from the beginning to April 2023. The search phrases used included "fetal fibronectin," "induced labour," "nulliparous women," "preterm labor," "labor induction," "vaginal delivery," and "cervical ripening." Additional studies were identified by manually scanning the reference lists of the retrieved papers. Upon critical searching the published literature, we did not get the RCTs on this study.
Study selection
The inclusion criteria for the studies encompassed the following: (1) they were designated as prospective observational studies, randomized controlled trials (RCTs), or cohort studies; (2) they assessed the predictive significance of fFN about the outcome of induced labor among nulliparous women; (3) they provided information on at least one of the following outcomes: success of labor induction, vaginal delivery rate, cesarean section rate, or duration of labor; and (4) they were published in the English language. The exclusion criteria for this study included the following: (1) studies conducted retrospectively; (2) studies that specifically examined multiparous women; (3) case reports, reviews, or meta-analyses; and (4) studies that did not provide outcomes of interest or lacked clear definitions of induced labor.
Data extraction
The data extracted encompassed various aspects of the study, such as its design, publication year, and setting. It also included participant demographics, including age and gestational age. Additionally, the data included information about the intervention and control groups, if applicable. The outcomes assessed in the study included the success of labor induction, vaginal delivery rate, cesarean section rate, and duration of labor. The main findings of the study, including statistics and p-values, were also included.
Quality assessment
The Newcastle-Ottawa Scale for cohort and case-control studies was used to evaluate the quality of the included studies. The assessment considered many forms of bias, including selection bias, performance bias, detection bias, attrition bias, and reporting bias.
Ethical considerations
Ethical clearance was deemed unnecessary for this systematic review since it included the synthesis of published data without the direct involvement of human participants. Nevertheless, it was anticipated that all research included in the analysis had acquired ethical clearance from their official institutional review boards.
Quality assessment of the observational studies
The quality of five observational studies is evaluated in Table 1 using the Newcastle-Ottawa Scale (NOS), which examines Selection, Comparability, and Outcome. The highest score assigned to these studies is 9 stars. Grab et al. (2022) [9], and Khalaf et al. (2023) [18] achieved flawless marks (9/9), so demonstrating their exceptional research design and implementation across all assessed areas. The Uygur et al. (2016) [19] and Reis et al. (2003) [20] received a score of 8 out of 9. However, there were fewer deductions in the areas of Comparability and Selection, suggesting potential issues in effectively controlling confounding factors and selecting appropriate cohorts. Sciscione et al. (2005) [21] achieved a flawless grade, indicating its thorough and rigorous methodology.
Bias assessment of the included studies
Table 2 presents a comprehensive evaluation of bias in the studies, using several criteria such as Selection, Performance, Detection, Attrition, and Reporting Bias to determine their overall integrity. Grab et al. (2022) [9], and Khalaf et al. (2023) [18] demonstrate a mostly low likelihood of bias. The Uygur et al. (2016) [19] and Sciscione et al. (2005) [21] have a moderate overall risk, mainly because of the significant influence of Performance Bias on the results. In contrast, the study conducted by the Reis et al. (2003) [20] demonstrates a notable prevalence of bias, mostly due to concerns related to Selection and Performance Bias, as well as major Attrition Bias.
Baseline characteristics of the included participants of each study
Table 3 investigates the prognostic significance of fetal fibronectin (fFN) and cervical length (CL) in predicting the outcomes of labor induction. The scope of the study encompasses prospective observational, which includes several participant groups, including nulliparous women and those undergoing labor induction. The interventions used in these investigations include fFN testing and assessments of CL, with the absence of designated control groups, hence highlighting the observational bias inherent in this study. The admission criteria exhibit variability, with a primary emphasis on pregnant women falling within particular gestational periods or possessing set Bishop scores. Conversely, the exclusion criteria often include the exclusion of multiparous women or those with contraindications to vaginal delivery. The outcomes focus on evaluating the effectiveness of labor induction, specifically analyzing the occurrence of spontaneous labor commencement and the rate of success in induced labor. These studies emphasize the usefulness of fFN and CL as crucial biomarkers for customizing labor induction techniques, emphasizing their contribution to improving obstetric care by strengthening the ability to predict labor outcomes.
Outcomes for the included studies
The examination of five research reveals the predictive importance of fetal fibronectin (fFN) in labor outcomes but with different levels of statistical significance as shown in Table 4. Sciscione et al. (2005) [21] and Uygur et al. (2016) [19] investigate the influence of fFN on the rates of vaginal birth and occurrences of cesarean section, respectively. Their findings demonstrate a noteworthy predictive significance of fFN in the latter (P = 0.002). In a study conducted by Reis et al. (2003) [20], the performance of fFN is compared to other predictors of labor induction. The results indicate that greater parity and Bishop scores are more reliable indicators of effective induction than fFN alone. The advantage of fFN over cervical length in predicting preterm delivery in twin pregnancies is emphasized in Grab et al. (2022) [9], but without particular statistical data. The high sensitivity, specificity, and accuracy of fFN in predicting effective labor induction are shown in Khalaf et al. (2023), with strong P-values providing evidence for this claim. Together, these trials highlight the usefulness of fFN in obstetric treatment, but there are subtle differences that need careful clinical interpretation.
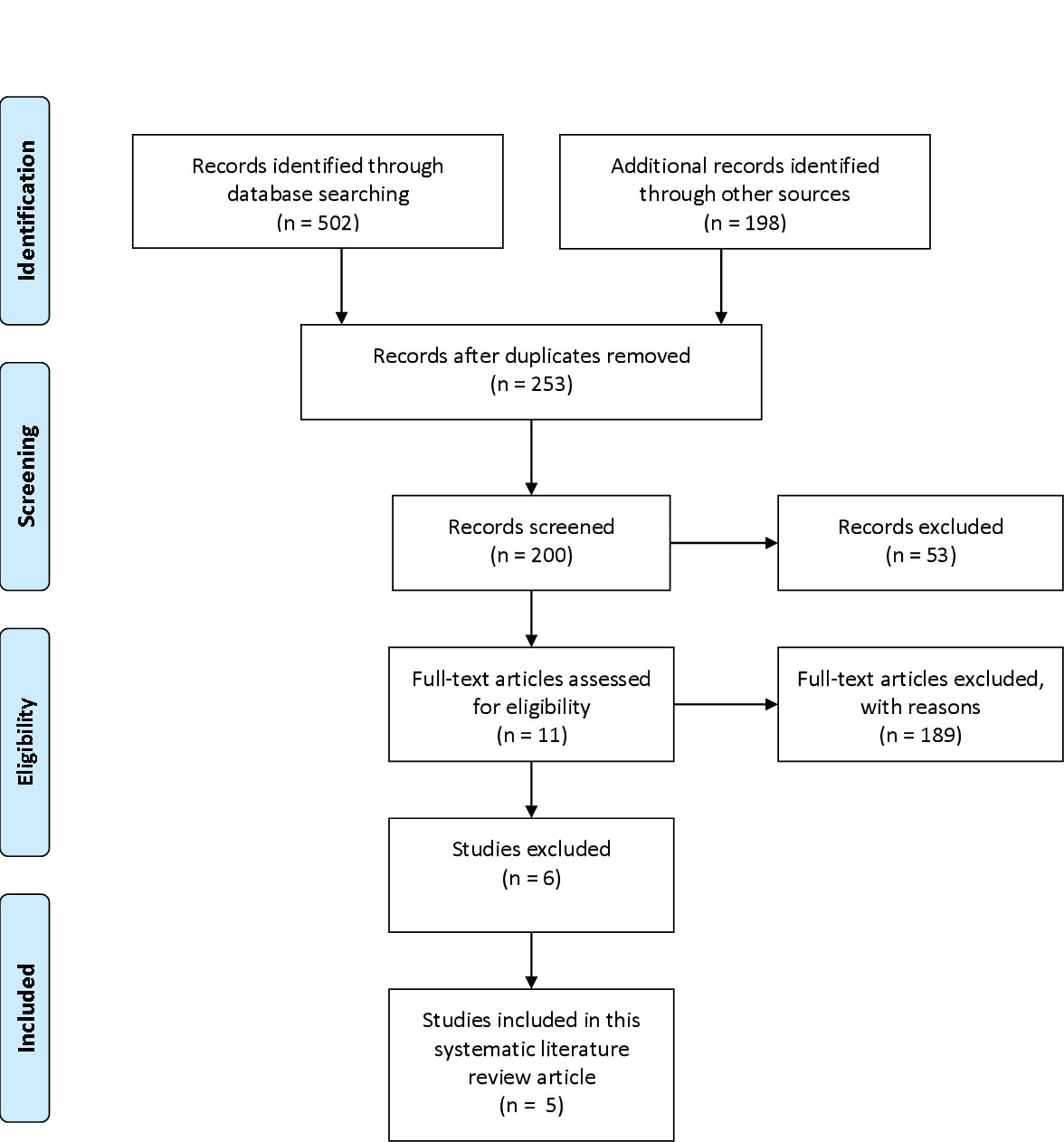 Figure 1. The PRISMA flow diagram for the included studies.
Figure 1. The PRISMA flow diagram for the included studies.
|
Table 1. Quality assessment of the observational studies. |
||||
|
Study ID |
Selection (4 Stars) |
Comparability (2 Stars) |
Outcome (3 Stars) |
Total (9 Stars) |
|
Grab et al. (2022) [1] |
★★★★ |
★★ |
★★★ |
9/9 |
|
Khalaf et al. (2023) [2] |
★★★★ |
★★ |
★★★ |
9/9 |
|
Uygur et al. (2016) [3] |
★★★★ |
★ |
★★★ |
8/9 |
|
Reis et al. (2003) [4] |
★★★ |
★★ |
★★★ |
8/9 |
|
Sciscione et al. (2005) [5] |
★★★★ |
★★ |
★★★ |
9/9 |
|
Table 2. Bias assessment of the included studies. |
||||||
|
Study ID |
Selection Bias |
Performance Bias |
Detection Bias |
Attrition Bias |
Reporting Bias |
The overall risk of Bias |
|
Grab et al. (2022) [1] |
Unclear |
Low |
Low |
Low |
Low |
Low |
|
Khalaf et al. (2023) [2] |
Low |
Low |
Low |
Unclear |
Low |
Low |
|
Uygur et al. (2016) [3] |
Low |
High |
Low |
Low |
Low |
Moderate |
|
Reis et al. (2003) [4] |
High |
High |
Low |
High |
Low |
High |
|
Sciscione et al. (2005) [5] |
Low |
High |
Low |
Low |
Low |
Moderate |
|
Table 3. Baseline characteristics of the included participants of each study. |
|||||||
|
Study ID |
Study Design |
Participants |
Intervention |
Control/Other |
Inclusion |
Exclusion |
Outcomes Assessed |
|
Grab et al. (2022) [1] |
POS |
268 |
fFN & CL measurement |
POS comparing outcomes based on fFN and CL measurements without a CG |
Pregnant women; specific gestational weeks not detailed |
Retrospective studies; non-English publications; studies without clear outcome measures |
Onset of labour within 5 days, the accuracy of fFN and CL in predicting labour |
|
Khalaf et al. (2023) [2] |
POS |
40 |
fFN & transvaginal ultrasonography for CL |
POS focusing on predictive values of fFN and cervical length without a distinct control group |
Nulliparous pregnant women, Bishop score ≤5 |
Multiparous women, retrospective studies, case reports, reviews, non-English publications |
Successful LI, sensitivity, specificity, and accuracy of fFN and CL measurement |
|
Uygur et al. (2016) [3] |
POS |
73 |
fFN assay to predict VD within 24 hours |
The study focuses on the predictive value of fFN |
Women undergoing LI |
N/A |
VD within 24 hours of LI |
|
Reis et al. (2003) [4] |
OS |
111 |
fFN testing and ultrasound parameters to predict LI |
OS comparing outcomes based on fFN presence |
Women undergoing LI |
N/A |
Association of fFN and ultrasound parameters with successful LI |
|
Sciscione et al. (2005) [5] |
OS |
241 |
pre-induction CR with an intracervical Foley catheter |
OS determines the effect of fFN on LI |
Nulliparous women undergoing pre-induction CR |
Contraindications to vaginal birth, previous cervical surgery, non-English publications |
Impact of fFN on duration of CR, oxytocin exposure, and LI |
|
Abbreviation: POS, Prospective Observational Study; OS, Observational Study; fFN, Foetal Fibronectin; CL, Cervical Length; CG, Control Group; LI, Labour Induction; VD, Vaginal Delivery; CR, Cervical Ripening. |
|||||||
|
Table 4. Outcomes for the included studies. |
||||
|
Study ID |
Outcomes Assessed |
Complications/Risk Factors |
Statistics |
P-Values |
|
Sciscione et al. (2005) [1] |
VD in nulliparous women |
No significant difference in VD rates between positive and negative fFN |
Positive fFN: 55.8% vs. Negative fFN: 53.3% |
P > .70 (vaginal), P > .56 (cervical) |
|
Uygur et al. (2016) [2] |
Success of LI within 24 hours |
Higher cesarean section rate in patients with negative fFN results |
Positive fFN: 84.8% (vd within 24 hours), Negative fFN: 72% (caesarean section) |
P = 0.002 (positive vs. negative fFN for VD) |
|
Reis 2003 [3] |
Successful induction of labor |
Higher parity, previous VD, higher Bishop scores, and shorter cervix were significantly associated with delivery within 24 hours; fFN test had poor performance |
Positive predictive value (PPV), negative predictive value (NPV), sensitivity, and specificity for various tests including fFN |
P = .021 (funneling present), P = .157 (fFN presence) |
|
Grab et al. (2022) [4] |
Prediction of preterm birth in twin pregnancies |
The superiority of fFN test over cervical length measurement in predicting preterm birth |
Not specified |
Not specified |
|
Khalaf et al. (2023) [5] |
Successful LI, sensitivity, specificity, and accuracy of fFN and CL measurement |
fFN showed high sensitivity, specificity, and accuracy in predicting successful LI |
Sensitivity: 85%, Specificity: 80%, Accuracy: 82.6% for fFN in predicting successful LI |
P < .05 for Bishop score relation with fFN, P = 0.029* for positive vs. negative fFN |
|
Abbreviation: VD, Vaginal Delivery; fFN, Foetal Fibronectin; CL, Cervical Length. |
||||
Sciscione et al. (2005) [21] study and Uygur et al. (2016) [19] research emphasizes the intricate significance of fFN in forecasting vaginal delivery rates and the probability of cesarean sections. These findings are consistent with previous research conducted by Ikeoha et al., (2022), which also identified fFN as a significant indicator of labor induction results [22]. The disparity in the predicted efficacy of fFN between the research and our own underscores the intricate nature of labor induction procedures and the varied function of fFN.
The Reis et al. (2003) [20] research contributes to the existing body of knowledge by conducting a comparative analysis of the prediction effectiveness of fFN about other well-established indicators such as parity and Bishop scores. The present comparative research demonstrates that the predictive value of fFN is substantial; yet, its success is dependent on a complex interaction of several clinical and physiological characteristics. Jun et al. (2019) support this discovery by advocating for a comprehensive strategy to labor induction that considers many factors to maximize results [10].
Grab et al. (2022) [9] research reveals that fFN is more effective in predicting outcomes in some situations, such as twin pregnancies, indicating its potential for customized use in obstetric treatment. The present conclusion is of particular interest when compared to the existing body of research, which often engages in disputes over the applicability of fFN's prognostic powers in various pregnancy scenarios [23].
Khalaf et al. (2023) [18] significantly contributes to this discourse by demonstrating the high sensitivity, specificity, and accuracy of fFN in predicting successful labor induction. This resonates with the assertions by Amro et al. (2023), highlighting fFN's robustness as a predictive tool [24]. Nonetheless, this study, alongside others reviewed, underscores the critical need for individualized assessment in applying fFN measurements, echoing the sentiments of Cornelissen et al. (2020) regarding personalized obstetric care [25].
Our comprehensive assessment of these studies confirms the crucial significance of fFN in predicting labor induction outcomes and highlights the varying effectiveness of fFN in various clinical situations. The presence of variability highlights the significance of including fFN measures in a thorough clinical evaluation framework. This approach ensures that choices about labor induction are based on full knowledge of the individual obstetric profile of each patient.
Furthermore, the systematic review highlights a significant deficiency in the current body of research on the continuous evaluation of fFN levels throughout pregnancy and their ability to predict outcomes at different stages of pregnancy. The existence of this vacuum in the literature provides an opportunity for further investigation, which may provide a novel understanding on the temporal patterns of fFN's predictive capacities.
Limitations
1. The primary emphasis of the review is on research conducted on women who have not given birth, which may restrict the applicability of the results to populations with multiple pregnancies or those with diverse obstetric backgrounds.
2. The inclusion of studies that use multiple designs and methodologies has the potential to increase heterogeneity, hence introducing complexities in the synthesis of results and inter-study comparisons.
3. The possibility for publication bias exists in the review, as studies that provide favorable findings are more likely to be published compared to those that yield negative or equivocal results. This bias has the potential to distort the overall comprehension of the predictive usefulness of fFN.
4. Restricting the review to papers written in English may exclude pertinent results published in other languages, so diminishing the scope of evidence considered and perhaps disregarding significant contributions to the field.
2. Advocate for policies that prioritize individualized care approaches, including fFN measures in conjunction with other clinical criteria to guide decision-making during labor induction.
3. Promote the allocation of more financial resources and assistance for collaborative research that specifically targets the enhancement of fFN prediction models.
4. Revise the current clinical guidelines to include evidence-based advice on the use of fFN testing, to enhance mother and newborn outcomes in cases of induced labour.
2. The fFN measurement may be used by healthcare practitioners to customize conversations with patients about the time and techniques of labor induction, which may lead to a decrease in the need for cesarean sections and an improvement in the safety of both mothers and newborns.
3. Develop and execute educational programs targeting healthcare professionals to augment their comprehension of the clinical manifestation associated with fFN testing.
2. Establish and implement uniform reporting criteria for fFN levels and labor outcomes, enabling easier comparisons across research and improving meta-analytic efforts.
3. Perform longitudinal research to investigate changes in fFN levels throughout pregnancy and their ability to predict outcomes at various stages of gestation, providing a more profound understanding of the timing and handling of labor induction.
4. To guide policy and practice, it is essential to assess the cost-effectiveness of incorporating fFN testing into standard prenatal care. This evaluation should consider the possible enhancement of labor outcomes as well as the economic ramifications for healthcare systems.
We extend our gratitude to all the students who participated in this research.
Ethics approval
As the project was a review article no ethical approval was needed.
Data availability
All relevant data are within the paper.
Funding
The authors did not receive any funding or support to report.
Authors’ contribution
FI: article conceptualization, article writing, data collection and proofreading, review for language check, formatting the article; IT: article conceptualization, article writing, and data analysis; NB: article conceptualization, article writing, data analysis, review for language check, formatting the article; FU: data collection, data analysis, and proofreading; HA: article conceptualization, article writing, proof reading, software analysis, supervising the study.
Competing interests
The authors have declared that no competing interest exist.
- ACOG Publications: January 2021. Obstetrics & Gynecology 2021, 137(1).
- Wooding DJ, Das P, Tiwana S, Siddiqi J, Khosa F: Race, ethnicity, and gender in academic obstetrics and gynecology: 12-year trends. Am J Obstet Gynecol MFM 2020, 2(4): 100178.
- Eden RD, Evans MI, Britt DW, Evans SM, Gallagher P, Schifrin BS: Combined prenatal and postnatal prediction of early neonatal compromise risk. J Matern Fetal Neonatal Med 2021, 34(18): 2996-3007.
- Berghella V: Attack on coronavirus disease 2019 from American Journal of Obstetrics & Gynecology MFM. Am J Obstet Gynecol MFM 2020, 2(2): 100119.
- Bolte EE, Moorshead D, Aagaard KM: Maternal and early life exposures and their potential to influence development of the microbiome. Genome medicine 2022, 14(1): 4.
- Reicher L, Fouks Y, Yogev Y: Cervical Assessment for Predicting Preterm Birth—Cervical Length and Beyond. J Clin Med 2022, 10(4): 627.
- Liu Y-S, Lu S, Wang H-B, Hou Z, Zhang C-Y, Chong Y-W, Wang S, Tang W-Z, Qu X-L, Zhang Y: An evaluation of cervical maturity for Chinese women with labor induction by machine learning and ultrasound images. BMC Pregnancy and Childbirth 2023, 23(1): 737.
- Beshir YM, Kure MA, Egata G, Roba KT: Outcome of induction and associated factors among induced labours in public Hospitals of Harari Regional State, Eastern Ethiopia: A two years' retrospective analysis. PLoS One 2021, 16(11): e0259723.
- Grab D, Doroftei B, Grigore M, Nicolaiciuc OS, Anton SC, Simionescu G, Maftei R, Bolota M, Ilea C, Costachescu G et al: Fetal Fibronectin and Cervical Length as Predictors of Spontaneous Onset of Labour and Delivery in Term Pregnancies. Healthcare (Basel) 2022, 10(7): 1349.
- Jun SY, Lee JY, Kim HM, Kim MJ, Cha HH, Seong WJ: Evaluation of the effectiveness of foetal fibronectin as a predictor of preterm birth in symptomatic preterm labour women. BMC Pregnancy Childbirth 2019, 19(1): 241.
- Centra M, Coata G, Picchiassi E, Alfonsi L, Meniconi S, Bini V, Di Tommaso M, Cozzolino M, Facchinetti F, Ferrari F et al: Evaluation of quantitative fFn test in predicting the risk of preterm birth. J Perinat Med 2016, 45(1): 91-98.
- Wang J, Cao Y, Chen L, Tao Y, Huang H, Miao C: Influence factor analysis and prediction model of successful application of high-volume Foley Catheter for labor induction. BMC Pregnancy and Childbirth 2023, 23(1): 776.
- de Vaan MD, Ten Eikelder ML, Jozwiak M, Palmer KR, Davies-Tuck M, Bloemenkamp KW, Mol BWJ, Boulvain M: Mechanical methods for induction of labour. Cochrane Database Syst Rev 2019, 10(10): Cd001233.
- Hong J, Atkinson J, Roddy Mitchell A, Tong S, Walker SP, Middleton A, Lindquist A, Hastie R: Comparison of Maternal Labor-Related Complications and Neonatal Outcomes Following Elective Induction of Labor at 39 Weeks of Gestation vs Expectant Management: A Systematic Review and Meta-analysis. JAMA Network Open 2023, 6(5): e2313162-e2313162.
- Slade L, Digance G, Bradley A, Woodman R, Grivell R: Change in timing of induction protocol in nulliparous women to optimise timing of birth: results from a single centre study. BMC Pregnancy and Childbirth 2022, 22(1): 316.
- Berghella V, Saccone G: Fetal fibronectin testing for reducing the risk of preterm birth. Cochrane Database Syst Rev 2019, 7(7): Cd006843.
- Gondane P, Kumbhakarn S, Maity P, Kapat K: Recent Advances and Challenges in the Early Diagnosis and Treatment of Preterm Labor. Bioengineering 2024, 11(2): 161.
- Khalaf WM, Abulnour AA, Mohamed ME, Elhamy HM, Saleh AM: Comparison between Fetal Fibronectin Versus Ultrasonographic Assessment of The Cervical Length in Patients with Unfavourable Cervix in Prediction of Successful Induction of Labor. Egyptian J Hosp Med 2023, 92(1): 6501- 6507.
- Uygur D, Ozgu-Erdinc AS, Deveer R, Aytan H, Mungan MT: Fetal fibronectin is more valuable than ultrasonographic examination of the cervix or Bishop score in predicting successful induction of labor. Taiwanese Journal of Obstetrics and Gynecology 2016, 55(1): 94-97.
- Reis FM, Gervasi MT, Florio P, Bracalente G, Fadalti M, Severi FM, Petraglia F: Prediction of successful induction of labor at term: role of clinical history, digital examination, ultrasound assessment of the cervix, and fetal fibronectin assay. Am J Obstet Gynecol 2003, 189(5): 1361-1367.
- Sciscione A, Hoffman MK, DeLuca S, O’Shea A, Benson J, Pollock M, Vakili B: Fetal Fibronectin as a Predictor of Vaginal Birth in Nulliparas Undergoing Preinduction Cervical Ripening. Obstetrics & Gynecology 2005, 106(5 Part 1).
- Ikeoha CC, Anikwe CC, Umeononihu OS, Okorochukwu BC, Mamah JE, Eleje GU, Ezeama CO, Nwokoye BI, Okoroafor CF, Ugwoke IS: Fetal Fibronectin as a Predictor of Preterm Delivery: A Nigerian Cohort Study. Biomed Res Int 2022, 2022: 2442338.
- Khan W, Zaki N, Ghenimi N, Ahmad A, Bian J, Masud MM, Ali N, Govender R, Ahmed LA: Predicting preterm birth using explainable machine learning in a prospective cohort of nulliparous and multiparous pregnant women. PLoS One 2023, 18(12): e0293925.
- Amro B, Alhalabi I, George A, Haroun H, Khamis AH, Sawalhi NA: Using Fetal Fibronectin Test to Reduce Hospital Admissions with Diagnosis of Preterm Labor: An Economic Evaluation Study. J Pers Med 2023, 13(6): 894.
- Cornelissen LGH, van Oostrum NHM, van der Woude DAA, Rolf C, Porath MM, Oei SG, van Laar J: The diagnostic value of fetal fibronectin testing in clinical practice. J Obstet Gynaecol Res 2020, 46(3): 405-412.
Asia-Pacific Journal of Surgical & Experimental Pathology
ISSN 2977-5817 (Online)
 Copyright © Asia Pac J Surg Exp & Pathol. This
work is licensed under a Creative Commons AttributionNonCommercial-No Derivatives 4.0 International (CC BY-NC-ND 4.0)
License.
Copyright © Asia Pac J Surg Exp & Pathol. This
work is licensed under a Creative Commons AttributionNonCommercial-No Derivatives 4.0 International (CC BY-NC-ND 4.0)
License.