
 Submit Manuscript
Submit Manuscript
Research Article | Open Access
The relationship between vitamin D, chronic kidney disease, and mineral and bone disorder: a complex interplay comprehensive review
Abdul Ghaffar1, Ghulam Mustafa2, Abdul Wahid3
1Department of Pharmacology, Faculty of Pharmacy and Health Sciences University of Balochistan, Quetta, Pakistan.
2Department of Pharmaceutics, Faculty of Pharmacy and Health Sciences University of Balochistan, Quetta, Pakistan.
3Department of Pharmacy Practice, Faculty of Pharmacy and Health Sciences University of Balochistan, Quetta, Pakistan.
Correspondence: Abdul Wahid (Department of Pharmacy Practice, Faculty of Pharmacy and Health Sciences, University of Balochistan, Quetta, Pakistan; E-mail: wahiduob@gmail.com).
Asia-Pacific Journal of Surgical & Experimental Pathology 2024, 1: 22-27. https://doi.org/10.32948/ajsep.2024.05.20
Received: 07 May 2024 | Accepted: 01 Jun 2024 | Published online: 09 Jun 2024
Key words CKD, MBD, Vit-D, PTH, metabolism, hypertension
CKD affects millions of people worldwide, with an estimated global prevalence of 8-16%, depending on the diagnostic criteria used [3]. This translates to hundreds of millions of individuals living with CKD. The risk of CKD increases with age, and it is a significant comorbidity in conditions like diabetes and hypertension [4]. The global burden of CKD is substantial, with associated healthcare costs exceeding $1 trillion USD annually. Rising mortality rates highlight the seriousness of CKD, with cardiovascular disease being a major cause of death in CKD patients. Early diagnosis and management are crucial to slow disease progression and prevent complications [5].
Chronic Kidney Disease (CKD) is categorized into five stages based on the estimated glomerular filtration rate (eGFR), which indicates the kidneys' filtering ability. The stages are as follows:
Stage 1: Mild decrease in kidney function (eGFR 90-60 mL/min/1.73 m²);
Stage 2: Moderate decrease in kidney function (eGFR 59-30 mL/min/1.73 m²);
Stage 3: Moderate to severe decrease in kidney function (eGFR 29-15 mL/min/1.73 m²);
Stage 4: Severe decrease in kidney function (eGFR 14-9 mL/min/1.73 m²);
Stage 5: Kidney failure (eGFR <9 mL/min/1.73 m²) necessitating dialysis or kidney transplantation [6].
Synthesis: Ultraviolet B (UVB) rays from sunlight penetrate the skin and trigger the production of vitamin D3 (cholecalciferol) in the epidermis.
Hydroxylation: Vitamin D3 is transported to the liver where it undergoes the first hydroxylation step by 25-hydroxylase, converting it to 25-hydroxyvitamin D (25(OH) D). This form serves as the major storage and circulation form of vitamin D in the body.
Activation: The final activation step occurs in the healthy kidneys. The enzyme 1-alpha-hydroxylase converts 25(OH) D into the biologically active form, 1, 25-dihydroxyvitamin D (1, 25(OH) 2D).
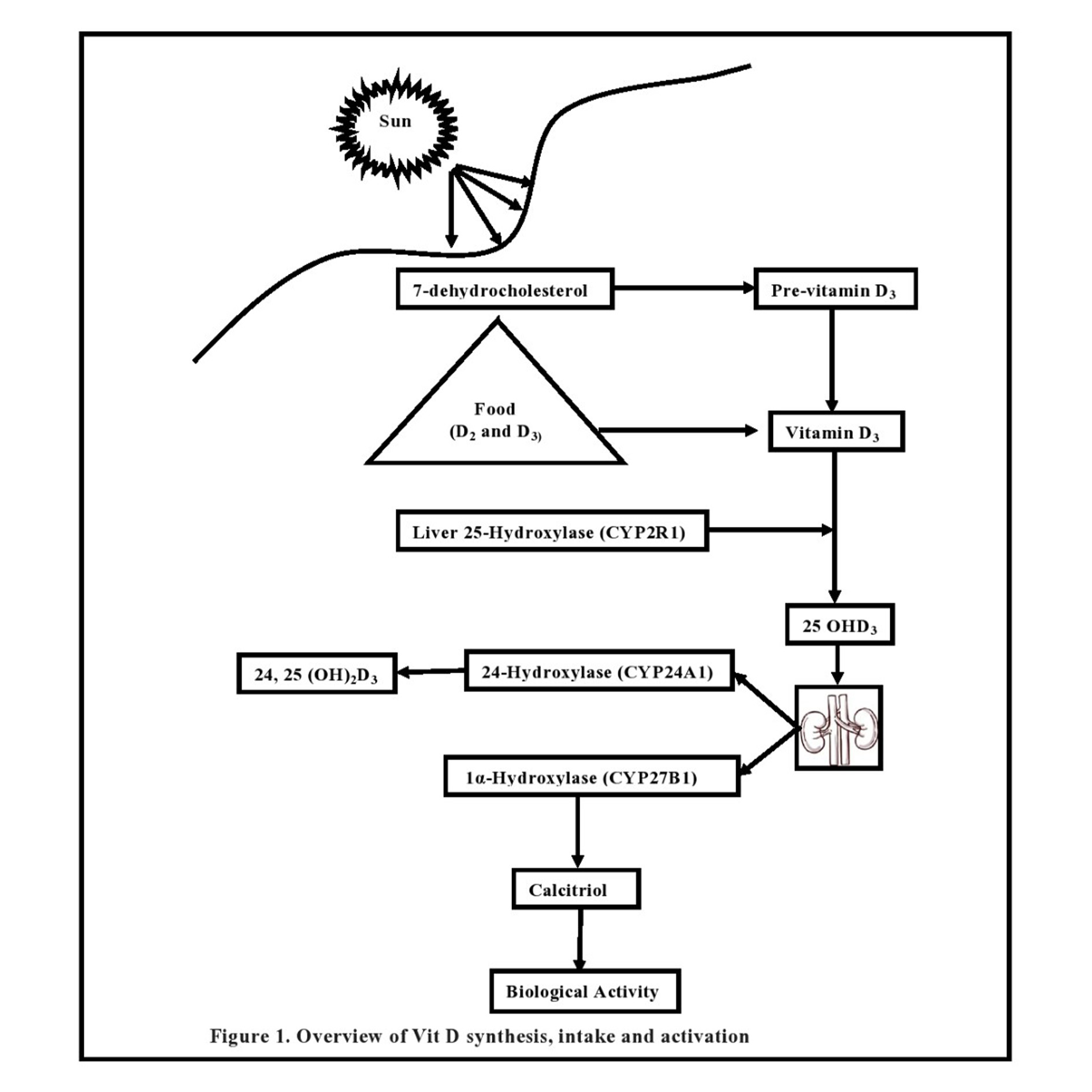 Figure 1. Flow chart of study participants evaluated for neck pain among smartphone users.
Figure 1. Flow chart of study participants evaluated for neck pain among smartphone users.
Impact on bone health
Several studies have investigated the effect of Vitamin D supplementation on BMD in CKD patients. Here's a summary with key findings and limitations:
Randomized controlled trials (RCTs) by Theobald et al. (2010) [21] and Locatelli et al. (2002) [22] demonstrated improvements in BMD with supplementation compared to placebo. These studies suggest that Vitamin D may promote bone mineralization and potentially slow bone loss in CKD patients.
A meta-analysis by Mathieu et al. (2017) [23] found limited evidence for significant overall BMD improvements across various studies. Heterogeneity in study design (dosage, duration), baseline vitamin D levels, and patient populations contribute to these inconsistencies (Figure 2).
Larger, well-designed RCTs with standardized protocols and longer follow-up periods are needed to definitively assess the impact of Vitamin D supplementation on BMD in CKD populations.
The Observational studies suggest an association between Vitamin D deficiency and increased fracture risk in CKD patients [24]. However, RCTs haven't shown consistent benefits. Studies by Locatelli et al. (2002) [22] and Manolagas et al. (2008) [25] haven't consistently shown a reduction in fracture risk with Vitamin D supplementation in CKD patients. Reasons for inconsistent findings in RCTs may include insufficient sample size, follow-up duration, and variations in baseline fracture risk or medication use amongst participants [26]. Further research exploring optimal dosing strategies, combination therapies with other medications, and targeting specific patient subgroups at high fracture risk is warranted to elucidate the potential benefits of Vitamin D for fracture prevention in CKD [26].
Impact on mineral homeostasis
Vitamin D supplementation can increase serum calcium levels in CKD patients due to its effect on intestinal calcium absorption [27]. Close monitoring of serum calcium levels is essential to avoid hypercalcemia, a potential side effect of supplementation, particularly in patients with pre-existing hypercalcemia or at risk of developing it. This may necessitate adjusting the Vitamin D dose or using calcium-binding medications [27]. The evidence regarding the impact of Vitamin D supplementation on phosphate levels in CKD remains mixed: Studies by Locatelli et al. (2002) [20] and Molnar et al. (2013) [28] show contrasting findings, with some suggesting potential benefits in lowering phosphate levels and others showing no significant effect.
Vitamin D's primary influence on phosphate metabolism is likely indirect, mediated through its effect on calcium and para thyroid hormone (PTH) levels. By promoting calcium absorption and suppressing PTH secretion, Vitamin D may indirectly contribute to lower phosphate levels [29]. More research is needed to explore the mechanisms by which Vitamin D supplementation might influence phosphate levels and its potential long-term impact on CKD-MBD management [29]. Some studies suggest that Vitamin D supplementation can contribute to PTH suppression in CKD patients [30]. Because Vitamin D promotes calcium absorption, reducing the need for PTH secretion by the parathyroid glands to maintain calcium homeostasis. Supplementation can help normalize PTH levels, potentially mitigating the detrimental effects of secondary hyperparathyroidism on bone health and cardiovascular function in CKD [30]. Studies like Henrich et al. (2011) [31] have shown that Vitamin D supplementation in conjunction with standard CKD-MBD treatment protocols can lead to a more significant reduction in PTH levels compared to placebo.
Impact on other aspects of CKD management
While the primary focus of Vitamin D supplementation in CKD is on improving bone health and mineral homeostasis in MBD, there's growing interest in its potential impact on other aspects of CKD management:
Vitamin D deficiency has been linked to muscle weakness and impaired physical function in various populations. Studies like Cessation of Dialysis Trialists' Collaborative Group (2010) [32] suggest that Vitamin D supplementation in dialysis patients may improve muscle strength and function. However, more research is required to confirm these findings and elucidate the underlying mechanisms.
CKD patients are at high risk for cardiovascular complications. Vitamin D's potential anti-inflammatory and vascular protective effects are being explored [33]. Observational studies suggest an association between Vitamin D deficiency and cardiovascular events in CKD. However, RCTs haven't yet established a definitive cause-and-effect relationship regarding Vitamin D supplementation and improved cardiovascular outcomes in this population [34]. Further research is necessary to determine if Vitamin D supplementation can contribute to a comprehensive cardiovascular risk reduction strategy in CKD.
Vitamin D's role in modulating the immune system is well recognized. CKD patients have a higher susceptibility to infections. Studies are underway to explore whether Vitamin D supplementation can enhance immune function and reduce infection risk in CKD, but more research is needed to establish conclusive evidence [35].
Vitamin D supplementation regimens and considerations
Given the complexities discussed above, determining the optimal Vitamin D supplementation regimen for CKD patients requires careful consideration of several factors:
Measuring serum 25(OH) D levels is crucial to assess Vitamin D status and guide supplementation decisions. Most experts recommend targeting sufficient levels (>30 ng/mL) for optimal bone and overall health in CKD patients [34]. Vitamin D supplementation regimens for CKD patients typically involve higher doses compared to the general population due to impaired kidney activation and increased needs. However, individualized dosing based on baseline vitamin D levels, response to therapy, and potential risks of hypercalcemia is essential [34].
In some cases, activated vitamin D analogs like alfacalcidol (1-alpha-hydroxyvitamin D3) may be prescribed by nephrologists to address vitamin D deficiency and its effects on calcium and PTH levels in CKD patients with severely impaired kidney function [35]. Regular monitoring of serum calcium, phosphate, and PTH levels is necessary during Vitamin D supplementation to ensure safety and adjust the regimen as needed.
The Vitamin D supplementation is often incorporated into a comprehensive CKD-MBD treatment plan that may include calcium-regulating binders, phosphate binders, and medications to manage PTH levels.
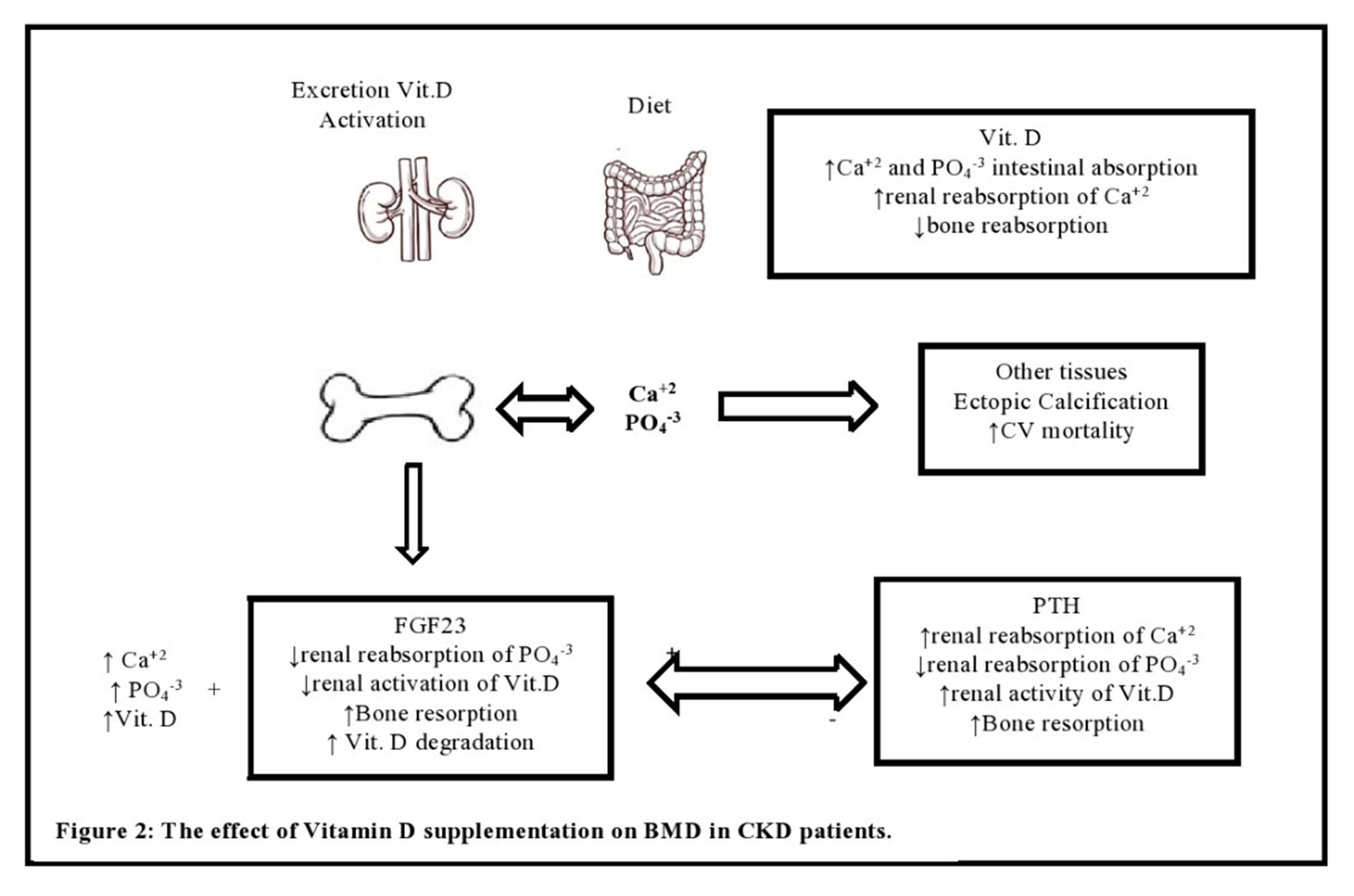 Figure 2. Prevalence of neck pain among smart phone users.
Figure 2. Prevalence of neck pain among smart phone users.
By addressing these knowledge gaps, healthcare professionals can refine Vitamin D supplementation strategies and optimize patient care in CKD management.
No applicable.
Ethics approval
No applicable.
Data availability
The Data will be available upon request.
Funding
The authors did not receive any financial support from any organization for the submitted work.
Authors’ contribution
Abdul Wahid and Abdul Ghaffar both significantly contributed to the conception, design, and writing of this review article. Ghulam Mustafa led the literature search, while Abdul Ghaffar contributed to the critical revision and editing of the manuscript. Abdul Wahid read and approved the final version of the manuscript.
Competing interests
The authors have diligently stated that they have no conflicts of interest to report.
- Ettinger S, Feldman D, Lips P: Clinical consequences of vitamin D deficiency. Mayo Clin Proc 2007, 82(11): 1407-1420.
- Kovesdy CP: Epidemiology of chronic kidney disease: an update 2022. Kidney Int Suppl (2011) 2022, 12(1): 7-11.
- National Kidney Foundation: The ABCs of Chronic Kidney Disease. 2024.
- Fenta ET, Eshetu HB, Kebede N, Bogale EK, Zewdie A, Kassie TD, Anagaw TF, Mazengia EM, Gelaw SS: Prevalence and predictors of chronic kidney disease among type 2 diabetic patients worldwide, systematic review and meta-analysis. Diabetol Metab Syndr 2023, 15(1): 245.
- GBD Chronic Kidney Disease Collaboration: Global, regional, and national burden of chronic kidney disease, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet 2020, 395(10225): 709-733.
- No authors: Chapter 1: Definition and classification of CKD. Kidney Int Suppl (2011) 2013, 3(1): 19-62.
- Subbiah AK, Chhabra YK, Mahajan S: Cardiovascular disease in patients with chronic kidney disease: a neglected subgroup. Heart Asia 2016, 8(2): 56-61.
- Moe SM, Fawzi FA, Goodman WG, Weir MR: Mineral and bone disorders in chronic kidney disease. Am J Med Sci 2006, 332(1): 55-62.
- Kaufman MR, Coyne DW, Singh A: Secondary hyperparathyroidism. Clin J Am Soc Nephrol 2008, 3(Suppl 1): S155-S161.
- Melton LJ, Kanis JA: Fracture Risk and Skeletal Adaptation in Chronic Kidney Disease. J Am Soc Nephrol 2004, 15(8): 2024-2030.
- Habas E Sr, Eledrisi M, Khan F, Elzouki AY: Secondary Hyperparathyroidism in Chronic Kidney Disease: Pathophysiology and Management. Cureus 2021, 13(7): e16388.
- Holick MF: Vitamin D deficiency. N Engl J Med 2016, 374(26): 2460-2473.
- Bikle DD: Nonclassic actions of 1,25-dihydroxyvitamin D3. J Clin Endocrinol Metab 2009, 94(1): 26-34.
- Cannell JJ, Hollis BW, Zasloff EM, Pfeiffer CM, Grindel SH, Musgrave DT: Muscle weakness and vitamin D deficiency in elderly women. J Am Geriatr Soc 2008, 56(4): 624-628.
- Aranow C, Singer A, Cantorna MT: Vitamin D and the immune system. J Clin Invest 2010, 120(11): 3580-3583.
- Shalhoub V, Massry SG: Disorders of vitamin D metabolism in chronic renal disease. Kidney Int 2000, 58(2): 400-413.
- Priyadarshini G, Parameswaran S, Sahoo J, Selvarajan S, Rajappa M: Vitamin D deficiency in chronic kidney disease: Myth or reality? Clin Chim Acta 2021, 523: 35-37.
- Chandra P, Binongo JN, Ziegler TR, Schlanger LE, Wang W, Someren JT, Tangpricha V: Oral cholecalciferol treatment in chronic renal insufficiency. Endocr Pract 2008, 14(1): 10-17.
- Holt SG, Smith ER: Fetuin-A-containing calciprotein particles in mineral trafficking and vascular disease. Nephrol Dial Transplant 2016, 31(10): 1583-1587.
- Chandra P, Binongo JN, Ziegler TR, Schlanger LE, Wang W, Someren JT, Tangpricha V: Cholecalciferol (vitamin D3) therapy and vitamin D insufficiency in patients with chronic kidney disease: a randomized controlled pilot study. Endocr Pract 2008, 14(1): 10-17.
- Feng Z, Lu K, Ma Y, Liu F, Zhang X, Li H, Fu Y: Effect of a high vs. standard dose of vitamin D3 supplementation on bone metabolism and kidney function in children with chronic kidney disease. Front Pediatr 2022, 10: 990724.
- Milinković NLj, Majkić-Singh NT, Mirković DD, Beletić AD, Pejanović SD, Vujanić ST: Relation between 25(OH)-vitamin D deficiency and markers of bone formation and resorption in haemodialysis patients. Clin Lab 2009, 55(9-10): 333-339.
- Yano S, Sugimoto T, Tsukamoto T, Yamaguchi T, Hattori T, Sekita KI, Kaji H, Hattori S, Kobayashi A, Chihara K: Effect of parathyroidectomy on bone mineral density in hemodialysis patients with secondary hyperparathyroidism: possible usefulness of preoperative determination of parathyroid hormone level for prediction of bone regain. Horm Metab Res 2003, 35(4): 259-264.
- Kovesdy CP, Zittermann A, Malluche HH: What we know and what we don't know about vitamin D and chronic kidney disease. Kidney Int 2015, 87(3): 529-537.
- 25.Plotkin LI, Lezcano V, Thostenson J, Weinstein RS, Manolagas SC, & Bellido T: Connexin 43 is required for the anti‐apoptotic effect of bisphosphonates on osteocytes and osteoblasts in vivo. Journal of Bone and Mineral Research 23(11), 1712-1721.
- Zheng CM, Wu CC, Hung CF, Liao MT, Shyu JF, Hsu YH, Lu CL, Wang YH, Zheng JQ, Chang TJ, et al: Cholecalciferol Additively Reduces Serum Parathyroid Hormone Levels in Severe Secondary Hyperparathyroidism Treated with Calcitriol and Cinacalcet among Hemodialysis Patients. Nutrients. 2018, 10(2): 196.
- Bhan I, Powe CE, Berg AH, Ankers E, Wenger JB, Karumanchi SA, Thadhani RI: Bioavailable vitamin D is more tightly linked to mineral metabolism than total vitamin D in incident hemodialysis patients. Kidney Int 2012, 82(1): 84-89.
- Pan S, Yang K, Shang Y, Yu R, Liu L, Jin J, He Q: Effect of regulated vitamin D increase on vascular markers in patients with chronic kidney disease: A systematic review and meta-analysis of randomized controlled trials. Nutr Metab Cardiovasc Dis 2024, 34(1): 33-44.
- Cessation of Dialysis Trialists' Collaborative Group: Effect of Vitamin D Supplementation on Muscle Strength in Dialysis Patients: An Individual Patient Data Meta-Analysis. Am J Kidney Dis 2010, 56(4): 734-742.
- Christodoulou M, Aspray TJ, Schoenmakers I: Vitamin D Supplementation for Patients with Chronic Kidney Disease: A Systematic Review and Meta-analyses of Trials Investigating the Response to Supplementation and an Overview of Guidelines. Calcif Tissue Int 2021, 109(2): 157-178.
- Coladonato JA, Ritz E: Secondary hyperparathyroidism and its therapy as a cardiovascular risk factor among end-stage renal disease patients. Adv Ren Replace Ther 2002, 9(3): 193-199.
- Kovesdy CP, Zittermann A, Malluche HH: What we know and what we don't know about vitamin D and chronic kidney disease. Kidney Int 2015, 87(3): 529-537.
- Franca Gois PH, Wolley M, Ranganathan D, Seguro AC: Vitamin D Deficiency in Chronic Kidney Disease: Recent Evidence and Controversies. Int J Environ Res Public Health 2018, 15(8): 1773.
- Kaur G, Singh J, Kumar J: Vitamin D and Cardiovascular Disease in Chronic Kidney Disease. Pediatr Nephrol 2019, 34(12): 2509-2522.
- American Association of Kidney Patients: Vitamin D and Dialysis. [https://aakp.org] Accessed March 20, 24.
Asia-Pacific Journal of Surgical & Experimental Pathology
ISSN 2977-5817 (Online)
 Copyright © Asia Pac J Surg Exp & Pathol. This
work is licensed under a Creative Commons AttributionNonCommercial-No Derivatives 4.0 International (CC BY-NC-ND 4.0)
License.
Copyright © Asia Pac J Surg Exp & Pathol. This
work is licensed under a Creative Commons AttributionNonCommercial-No Derivatives 4.0 International (CC BY-NC-ND 4.0)
License.